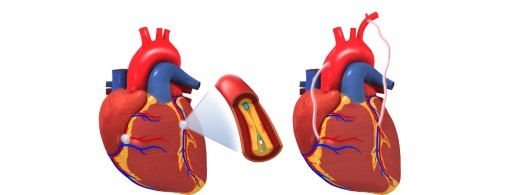
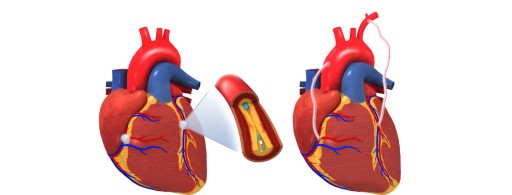
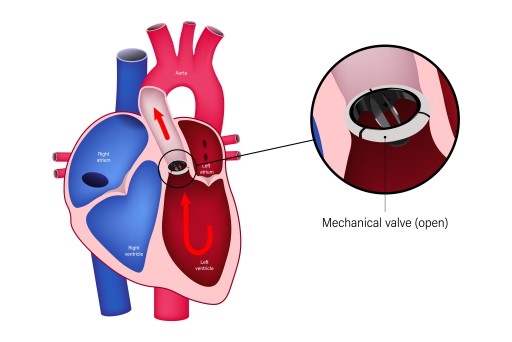
When the Heart Follows the LiverManaging Cardiac Surgeries in Hepatic CompromiseHIGH-RISK CABG IN A PATIENT WITH LIVER DYSFUNCTIONA 55-year-old gentleman with autoimmune hepatitis, chronic kidney disease, and previous CVA presented with rest angina. Coronary angiogram revealed triple vessel disease. Despite ascites and pulmonary hypertension, he underwent successful high-risk CABG performed by Dr. Srinath Vijayasekharan & Dr Senthil Kumar (Cardiothoracic and Heart & Lung Transplantation Surgeon). Intraoperatively, ischemic MR was noted but managed medically, and mitral valve replacement was avoided. The patient recovered without complications, reflecting a tailored approach to high-risk cardiac cases